Neck Lymph Nodes
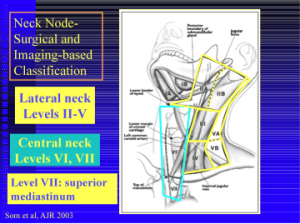
Neck Lymp Nodes Classification by Levels II-VII:
Current ATA guidelines state that low risk, stage I and II, Papillary thyroid cancer patients do not require radioiodine in most circumstances. This aggressive treatment is reserved for high risk patients in conjunction with Nuclear Medicine specialist.
Malignant Thyroid Nodule:

E. Radioactive Iodine (I-131)
I – 131 has been used for decades to treat hyperthyroidism and thyroid cancer. This is usually a one time treatment where you swallow a small capsule containing radioactive iodine. Since the thyroid is the only body part that uses iodine, I 131 is a targeted therapy to thyroid tissue alone. Dr. Hands oversees all I 131 treatments to ensure appropriate dosing and American Thyroid Association (ATA) guidelines are followed for the treatment of Graves and thyroid cancer.
F. Thyrogen (recombinant human TSH)
is an injection medication (buttocks) used to prepare thyroid cancer patients for I-131 ablation. It is administered on the two days prior to receiving I-131. By giving you TSH “stimulation” the remaining cancer cells after surgery are primed to receive I 131. Prior to the advent of Thyrogen, this was traditionally done by removing your thyroid hormone suppression (stopping levothyroxine or Synthroid) for weeks before treatment to make you significantly hypothyroid. With use of thyrogen, you may remain on your thyroid medication, live a normal life without the long standing ill effects of being hypothyroid for your treatment period.
Although not FDA approved for goiters, Thyrogen is used to facilitate the treatment of large nodular goiters with I-131, in place of surgery. This can reduce the size of the goiter without surgery in patients where surgery may be risky.
G. Thyroid Lab
CLIA certified to process blood samples for TSH, free T4 (Thyroxine), free T3 Thyroperoxidase (TPO) Antibodies, and Thyroglobulin (Tg) Antibodies. Thyroglobulin antigen (TgAg) and TgAg washes from lymph nodes are sent out to reference labs. Cytopath slides are also processed for adequacy and reviewed with thyroid cytopathologist.
Malignant nodule missed by non-thyroidologist performing US thyroid:


More Information
